
THI Doctors First to Describe an Uncommon Cause for Atypical Flutter
THI’s Clinical Cardiac Electrophysiology Research Team Discovers a Pattern of Macroreentrant Atrial Flutter Arising in Patients Who Underwent Transseptal Puncture
The Clinical Cardiac Electrophysiology Research group that includes Drs. Mehdi Razavi, Mohammad Saeed, and fellows Drs. Robert Paisley and Mitch Tan recently published a case series in Heart Rhythm Case Reports that calls attention to an important finding: an abnormal heart rhythm called atrial flutter arising in patients who have had procedures performed in the left atrium after a transseptal puncture. Transseptal puncture is a procedure in which a hole is surgically created in the wall between the left and right atria by using a long, curved needle and sheath placed from the groin to the heart. This allows catheters to pass from the right to the left side of the heart for cardiovascular procedures. To date, transseptal puncture has not been investigated as a potential cause of atrial flutter. However, these case study findings clearly suggest that this possibility merits further consideration.
Transseptal puncture is commonly used for various cardiac procedures, including atrial fibrillation ablation, transcatheter mitral valve repair, and certain types of left atrial appendage closure. At the site where the heart tissue is punctured to create the communication between the left and right atria, scar tissue may form over time and lead to the blockage of electrical signals passing in one direction, but not in the opposite direction. This electrical block can allow a continuous wave of electrical stimulation to travel in a circular motion around the transseptal puncture scar and perpetually activate the heart at a rate that is too fast (ie, tachycardia).
When the circuit creating the abnormal rhythm is in an area of heart muscle that is greater than a microscopic scale, it is referred to as “macroreentry” because the electrical signal continually “re-enters” the abnormal circuit to sustain the rhythm. Macroreentrant arrhythmias in the atria are termed “flutter” because of the undulating pattern of electrical activation seen on the electrocardiogram.
Patients with atrial flutter may feel a racing heartbeat, lightheadedness, shortness of breath, or fatigue. If untreated and uncontrolled over an extended period of time, atrial flutter can deteriorate heart muscle function and cause heart failure. Although atrial flutter is common, it usually arises from places in the heart other than the septum. Because of the uncommon location of the transseptal puncture arrhythmia circuit, this problem can be difficult to identify. Ablation (ie, with burning or freezing) can be used to terminate the arrhythmia by stopping the conduction of electrical signal through the circuit and eliminating tachycardic symptoms.
In the case series by Paisley and colleagues, the three patients had two key things in common: 1) an atypical atrial flutter involving the septum and 2) a history of multiple prior transseptal punctures related to previous ablation procedures. These findings raise the following important considerations.
An increased number of transseptal punctures and the larger size of transseptal access sheaths may predispose patients to increased scar burden and therefore a greater propensity to develop this unusual arrhythmia. As mentioned above, transseptal puncture is widely used for a variety of procedures, most often for treating atrial fibrillation. Despite improved techniques and ablation technologies, repeat ablation procedures are expected to remain necessary, especially for patients with recurrent tachyarrhythmia. As of 2017, an estimated 75,000 ablation procedures for atrial fibrillation were performed annually. Approximately 28% of these patients are expected to require repeat atrial fibrillation ablation within 3 years of the first ablation procedure.
When formulating treatment plans for individuals with difficult to treat atrial flutter, arrhythmia arising from transseptal access is an increasingly important entity to consider. Patients with atrial septal flutters who do not undergo careful study may be assumed to have more common types of atrial flutter and undergo ineffective ablations directed at other regions of the heart. Early recognition that atrial flutter may arise from the septum in patients who have had multiple prior transseptal access procedures can expedite detection and effective treatment.
With these considerations in mind, electrophysiologists should be aware of the potential for atrial flutter to originate from the interatrial septum after repeated transseptal access. Future investigations are warranted that will help shed more light on possible ways to mitigate this phenomenon.
“These kinds of cases are rare, but knowing the pattern can help the physician treat them effectively in the EP lab, “said Mohamed Saeed, Program Director of the Texas Heart Institute Clinical Electrophysiology Fellowship at Baylor St. Luke’s Medical Center and Associate Professor of Medicine at Baylor College of Medicine.
Read Report
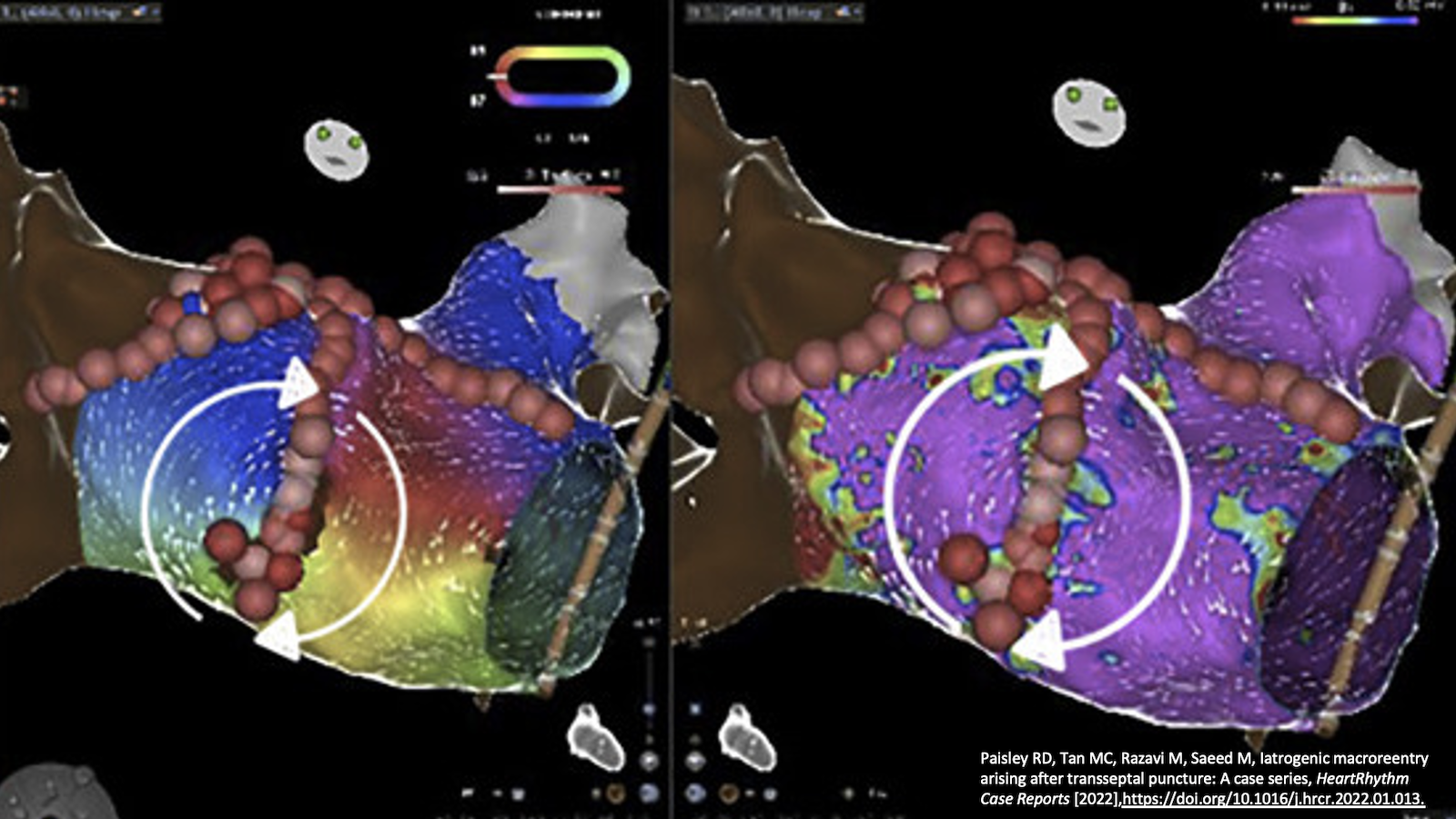
Paisley RD, Tan MC, Razavi M, Saeed M, Iatrogenic macroreentry arising after transseptal puncture: A case series, HeartRhythm Case Reports [2022], https://doi.org/10.1016/j.hrcr.2022.01.013.
News Story By Nicole Stancel, PhD, ElS(D)
Image : The ablation points are represented by circles in shades of gray, pink, and red. Red circles indicate a higher level of ablation time and energy, and gray-shaded circles indicate lower level of ablation time and energy. Arrows depict the electrical activation sequence. (Paisley RD, Tan MC, Razavi M, Saeed M, Iatrogenic macroreentry arising after transseptal puncture: A case series, HeartRhythm Case Reports [2022] Figure 3)

